实验概要
During more than 25 years of application in immunological sciences, ELISPOT has been established as a routine, robust, versatile, and reliable assay. From basic research to clinical immune monitoring, ELISPOT is being used to address the quantification and (to a lesser extent) functional characterization of immune cells secreting different molecules in the context of health and disease, immune intervention, and therapy in humans and other species [Kalyuzhny (Ed.) (2005) Handbook of Elispot: methods and protocols, Vol. 302, Humana Press Inc., Totowa, NJ]. Over the last decade, ELISPOT assays have been increasingly implemented as an immune-monitoring tool in clinical trials [Schmittel et al. J Immunother 23:289–295, 2000; Whiteside Immunol Invest 29:149–162, 2000; Nagata et al. Ann N Y Acad Sci 1037:10–15, 2004; Cox et al. (2005) Cellular immune assays for evaluation of vaccine efficacy in developing countries., In Manual of Clinical Immunology Laboratory (Rose, N. R., Hamilton, R. G., and Detrick, B., Eds.), p 301, ASM Press, Washington, DC; Cox et al. Methods 38:274–282, 2006]. While the principles of the original protocol have changed little since its first introduction [Czerkinsky J Immunol Methods 110:29–36, 1988], individual laboratories have adapted assay procedures based on experimental needs, availability of reagents and equipment, obtained recommendations, and gained experience, leading to a wide disparity of applied ELISPOT protocols with inevitable consequences. This chapter addresses the resulting challenges for ELISPOT use in clinical trial settings, and discusses the influence of harmonization strategies as a tool for overcoming these challenges. Furthermore, harmonization is discussed in the context of assay standardization and validation strategies.
实验原理
1. ELISPOT Assay: Achievements
The strength of the ELISPOT technique lies in its outstanding sensitivity to detect antigen-specific T and B cells in even very low frequencies, on a single cell level (8). In most scenarios, the assay can be performed without any in vitro expansion of cells or addition of exogenous cytokines, offering the possibility to attain a precise estimate of reactive cells in a donor. Further, these measurements can be achieved in relatively short time with a straightforward protocol that can be standardized and exposed to qualification and validation procedures following available guidance (9–11). The assay can be adapted to high-throughput sample screening which is supported by the demonstration that cryopreserved cells can perform comparable to fresh cells in ELISPOT assays (12). Further, a wide range of qualified reagents, materials, and equipment exists, and various controls and quality assurance parameters have been described and made available to scientists performing the assay (13–15). While the advantage of ELISPOT testing is its superb screening ability for cells secreting a specific cytokine (most commonly, IFN-γ), it has to be noted that it can be adapted to the simultaneous detection of two cytokines (16,17), as well as a variety of secreted molecules, including granzyme B (18) and perforin (19).
2. ELISPOT Assay: Challenges
As in every assay, the outcome is dependent on the protocol choices made (9) and the established laboratory environment the assay is conducted in (20). It is well-known and reviewed elsewhere that choices, like ELISPOT plate, antibody coating concentration, spot development system, and other protocol variables, can influence the final spot numbers (9). Further adding to possible sources of result variation is the final analysis approach of ELISPOT plates (21). Another complicating issue is the nonlinearity of responses in dependence of the cell number plated in a well. While linearity is preserved within a specific cell range (typically, <150,000 effector cells per well) if sufficient costimulation as well as antigen presentation by separate cells are provided, there is only a limited linearity range existent when peripheral blood mononuclear cells (PBMCs) are used as effectors and antigen presenters at the same time. This observation is most likely influenced by the fact that less than 200,000 PBMCs per well do not guarantee optimal antigen presentation conditions while more than 200,000 cells start to pile up on each other, thus providing good cell-to-cell contact, but limiting the percentage of cells with direct contact to the coating antibody bound to the well membrane, which is essential for spot formation.
These findings are not new, and the field has responded with the establishment of Standardized Operating Procedures (SOPs), especially in clinical immune-monitoring labs. During this process, labs typically test variations of different protocol choices and select those with the most desired outcome as the standard to adhere to. A logical conclusion would be that all standardized laboratories have similar protocols since it can be assumed that each one opted for the most desired results (highest specific spot numbers, lowest background reactivity levels, and lowest variability within replicates), which should be achievable with the most optimized reagents, materials, and general protocol procedures. Nonetheless, countless different SOPs exist, even for closely related experimental requirements. Certainly, some of this divergence can be explained by factors already mentioned earlier, like local availability or preference of reagents and materials and their vendors, previous experience of operators, or recommendations obtained from collaborators.
However, parts of this development might be accounted for by the predicament of the lack of a true gold reference standard for ELISPOT. Some groups attempt to solve this challenge by using T-cell lines or clones, others PBMC reference samples. While the first option is of limited wider applicability, the latter one does not truly represent a reference standard since the actual number of antigen-specific T cells able to secrete a given cytokine in these preparations is not precisely known. PBMC reference samples can be an excellent tool for standardization and validation approaches, as well as external controls for ELISPOT experiments; they are not, however, a reference standard for the amount of analyte or, in the case of ELISPOT, the number of antigen-specific cytokine-secreting cells. Hence, the question always remains: Is the measurement perceived as optimal with a given protocol indeed the correct measurement? Or with other words: Does the protocol permit optimal sensitivity and specificity (all cells detected without false-positive signals)?
The key question that arises from these challenges is: How comparable are ELISPOT measurements across laboratories?
实验材料
1. SOP for human IFN-γ ELISPOT assay.
2. PBMC.
3. CEF peptide pool (consisting of a panel of 8–11mers derived from Cytomegalovirus (CMV), Epstein–Barr virus (E BV), and Influenza virus (F lu) epitopes (14)).
4. CMV pp65 peptide pool (consisting of 15mers overlapping by 11 amino acids, spanning the entire protein (13)).
5. Ongoing ELISPOT proficiency panel program
实验步骤
1. The Dual Impact of Proficiency Panel Testing
Proficiency panel programs are typically conducted to provide participants a feedback about their test performance relative to a predefined reference value (see Note 1). This feedback can be of additional importance, as regular and successful (e.g., results within a given range) participation in proficiency panel programs might be requested by regulatory frameworks, depending on the specific setting.
In addition to quality assessment, proficiency panel programs can serve as a tool to define the extent and specifics of assay harmonization necessary. In order to allow the identification of critical assay steps that influence the assay outcome and to generate harmonization guidelines, proficiency panels need to be properly designed and conducted in such a way that a large enough number of representative data sets are obtained. Successful assay harmonization can first and foremost increase the comparability of results generated across institutions. This goal clearly is of high interest to the scientific community, but might not be the main interest of participating labs. Here, the question how individual labs can benefit from participating in harmonization activities is addressed.
2. Quality Assessment
It has been clearly stated that each method implemented for patient testing needs to undergo an external quality assessment via proficiency panel testing (22). For such testing, the same samples are sent to participating laboratories, where they need to be tested with the established assay. Results are centrally collected and analyzed. A feedback about each lab’s performance is given in comparison to the entire panel. If a lab’s performance is not in acceptable consensus with the overall panel results, necessary steps to correct and improve the assay outcome within that lab need to be taken.
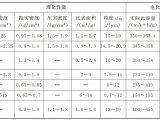
It has been suggested that the expected accuracy for proficiency panel testing should be >90% (22). However, as accuracy describes the closeness of results to the true value, determining the accuracy level for ELISPOT testing is a challenge due to the difficulty to ascertain the actual number of antigen-specific cells in PBMC samples. A solution to this impediment could be offered by the proficiency panel itself. Given a well-designed panel with a sufficient number of participating laboratories with their own established protocol (providing an acceptable cross-section of applied protocols in the field), it can be assumed that the measurement median of the entire panel for a given sample provides a representative estimate of antigen-reactive cells in that sample. In fact, an accumulation of participants’ measurements around the panel median has been demonstrated for previously conducted ELISPOT and other proficiency panels (Fig. 1) (23, 24). With this in mind, it appears reasonable to propose that the median measurement values of large, open panels could provide a range for an alternative reference standard for certain biological assays, like ELISPOT (see Note 2).

The use of ELISPOT assays as an immune-monitoring tool in clinical trial context has consequently led to the initiation of various large international proficiency panel programs (23,25,26). A main goal of these panels is to offer an external quality assessment for laboratories using ELISPOT for patient testing in the cancer and HIV vaccine and related fields. A central aspect of these programs is their thought-out design that allows comparability of results while including laboratories with different protocols in place. Not surprisingly, the interlaboratory variability observed was high, and labs were identified that were not able to detect all responses even on a yes/no basis. Recent harmonization efforts evolving out of these activities have dramatically improved these initial observations (see Subheading 3.3). Furthermore, panels with strict overall standardization as required in specific vaccine networks were able to demonstrate encouraging concordance of results (see Note 3) (27).
3. Assay Harmonization
Several smaller ELISPOT proficiency panels with a limited number of participating centers were conducted by groups in the field of cancer, autoimmunity, and infectious diseases (28–30). Larger, more systematic approaches to identify critical assay variables were initiated in 2005 and mainly driven by the HIV and cancer vaccine field (23, 25, 26, 31, 32).
The design of large international ELISPOT proficiency panels with the inclusion of labs employing different SOPs has opened the door to a process that allows the investigation of crucial protocol variables which influence the assay outcome in either direction. Once such variables have been identified, measures can be taken to harmonize the field toward a uniform approach of dealing with them. During the past few years, two collaborating programs have made significant contributions to the harmonization of ELISPOT testing: the proficiency panel program of the Cancer Immunotherapy Consortium of the Cancer Research Institute (CIC/CRI) and the Cancer Immunoguiding Program (CIP) of the Association for Cancer Immunotherapy (CIMT). Both programs were able to systematically investigate specific protocol variables for their influence on ELISPOT testing by analyzing data and protocol specifics obtained from their recurring large-scale proficiency panels. Their findings are summarized in initial ELISPOT harmonization guidelines which were made available to the community (23, 26). Interestingly, these initial guidelines address rather general assay steps, which do not require major protocol changes and, importantly, do not impose strict overall standardization measures to the field (Fig. 2). Most importantly, they are continuously being adapted by panelists, and their implementation has assisted remarkably in improving the overall panel outcome (Fig. 3) (33). Notably, these harmonization efforts do not end with the publication of initial guidelines, but continue with constant refinements (see Note 4). For instance, both programs have initiated a thorough investigation of the influence of serum and the use of serum-free media for the ELISPOT assay. It could be shown that serum is not required for ELISPOT performance (34) and that commercially available serum-free media can perform at least equally well in human IFN-γ ELISPOT assays as extensively pretested serum-supplemented media (35). A logical next study is underway testing the influence of different freezing media on ELISPOT outcome.




 首页
首页